Overpronation Of The Feet
Overview
The anatomy of a normal foot allows for both to occur at the same time. Approximately 30% of the population have a normal foot. The remainder of people either overpronate (95% of abnormal feet) or oversupinate (5% of abnormal feet). The important thing to know is that all feet pronate and supinate, but abnormal feet do one of these things too much or at the wrong time. When the foot overpronates or oversupinates, several foot ailments can develop.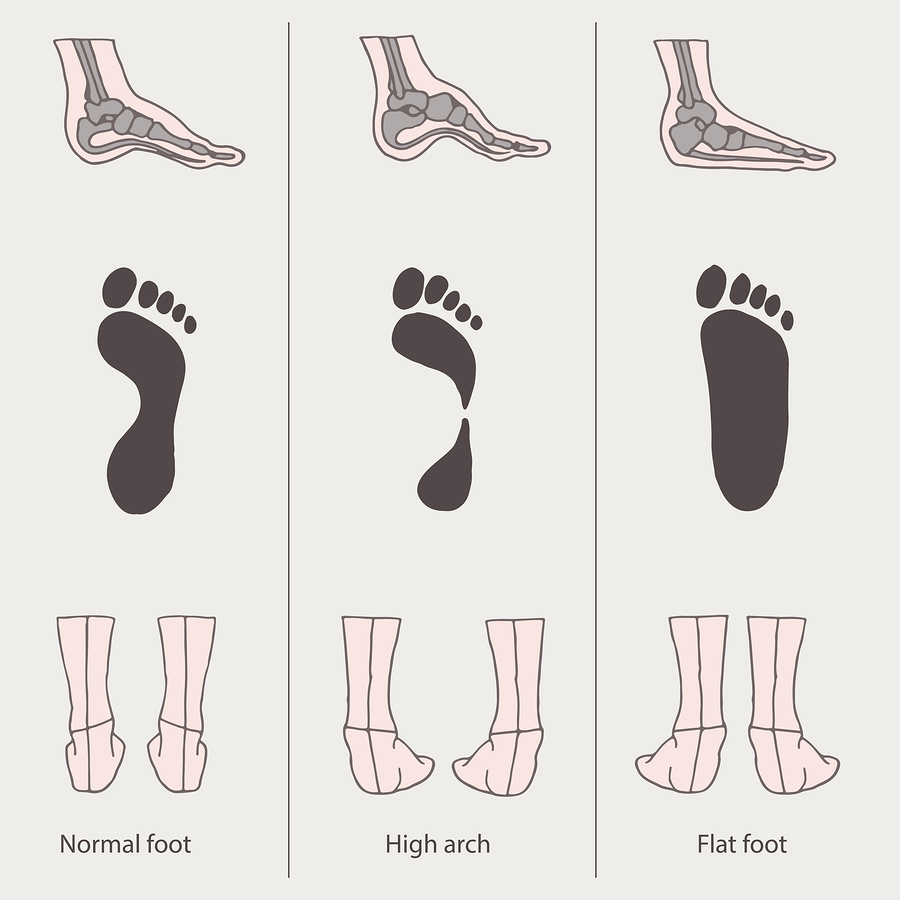
Causes
Abnormal foot biomechanics usually causes over-use type injuries, occurring most frequently in runners. When a neutral foot pronates during walking or running, the lower leg, knee and thigh all rotate internally (medially). When an athlete with an overpronated foot runs, this rotation movement is exaggerated and becomes more marked.
Symptoms
Symptoms can manifest in many different ways. Here is a list of some of the common conditions associated with over-pronation in children. Achilles Pain. Ankle pain. Arch Pain. Low back pain. Heel Pain. Knee Pain (Runner's knee and Chondromalecia of the patella) Osgood Schlatter Disease (pain below the knee) Shin Splints (pain in the front of the lower leg) Over-pronation does not necessarily mean your child has "flat feet." Even though children's arches may be relatively high when they lie down or sit, over-pronation may not be seen until your child is standing. A certain amount of pronation is normal. During normal walking or running ("gait cycle"), the heel strikes the ground and the foot rolls inward to absorb shock and adapt to the surface. This gait cycle is even more important if the running surface is uneven.
Diagnosis
To easily get an idea of whether a person overpronates, look at the position and condition of certain structures in the feet and ankles when he/she stands still. When performing weight-bearing activities like walking or running, muscles and other soft tissue structures work to control gravity's effect and ground reaction forces to the joints. If the muscles of the leg, pelvis, and feet are working correctly, then the joints in these areas such as the knees, hips, and ankles will experience less stress. However, if the muscles and other soft tissues are not working efficiently, then structural changes and clues in the feet are visible and indicate habitual overpronation.
Non Surgical Treatment
An orthotic is a device inserted inside the shoe to assist in prevention and/or rehabilitation of injury. Orthotics support the arch, prevent or correct functional deformities, and improve biomechanics. Prescription foot orthoses are foot orthoses which are fabricated utilizing a three dimensional representation of the plantar foot and are specifically constructed for an individual using both weightbearing and nonweightbearing measurement parameters and using the observation of the foot and lower extremity functioning during weightbearing activities. Non-prescription foot orthoses are foot which are fabricated in average sizes and shapes in an attempt to match the most prevalent sizes and shapes of feet within the population without utilizing a three dimensional representation of the plantar foot of the individual receiving the orthosis.
Prevention
Custom-made orthotics supports not only the arch as a whole, but also each individual bone and joint that forms the arch. It is not enough to use an over-the-counter arch support, as these generic devices will not provide the proper support to each specific structure of the arch and foot. Each pronated foot?s arch collapses differently and to different degrees. The only way to provide the support that you may need is with a custom-made device. This action of the custom-made orthotic will help to prevent heel spurs, plantar fasciitis, calluses, arch pain, and weakness of the entire foot.
The anatomy of a normal foot allows for both to occur at the same time. Approximately 30% of the population have a normal foot. The remainder of people either overpronate (95% of abnormal feet) or oversupinate (5% of abnormal feet). The important thing to know is that all feet pronate and supinate, but abnormal feet do one of these things too much or at the wrong time. When the foot overpronates or oversupinates, several foot ailments can develop.
Causes
Abnormal foot biomechanics usually causes over-use type injuries, occurring most frequently in runners. When a neutral foot pronates during walking or running, the lower leg, knee and thigh all rotate internally (medially). When an athlete with an overpronated foot runs, this rotation movement is exaggerated and becomes more marked.
Symptoms
Symptoms can manifest in many different ways. Here is a list of some of the common conditions associated with over-pronation in children. Achilles Pain. Ankle pain. Arch Pain. Low back pain. Heel Pain. Knee Pain (Runner's knee and Chondromalecia of the patella) Osgood Schlatter Disease (pain below the knee) Shin Splints (pain in the front of the lower leg) Over-pronation does not necessarily mean your child has "flat feet." Even though children's arches may be relatively high when they lie down or sit, over-pronation may not be seen until your child is standing. A certain amount of pronation is normal. During normal walking or running ("gait cycle"), the heel strikes the ground and the foot rolls inward to absorb shock and adapt to the surface. This gait cycle is even more important if the running surface is uneven.
Diagnosis
To easily get an idea of whether a person overpronates, look at the position and condition of certain structures in the feet and ankles when he/she stands still. When performing weight-bearing activities like walking or running, muscles and other soft tissue structures work to control gravity's effect and ground reaction forces to the joints. If the muscles of the leg, pelvis, and feet are working correctly, then the joints in these areas such as the knees, hips, and ankles will experience less stress. However, if the muscles and other soft tissues are not working efficiently, then structural changes and clues in the feet are visible and indicate habitual overpronation.
Non Surgical Treatment
An orthotic is a device inserted inside the shoe to assist in prevention and/or rehabilitation of injury. Orthotics support the arch, prevent or correct functional deformities, and improve biomechanics. Prescription foot orthoses are foot orthoses which are fabricated utilizing a three dimensional representation of the plantar foot and are specifically constructed for an individual using both weightbearing and nonweightbearing measurement parameters and using the observation of the foot and lower extremity functioning during weightbearing activities. Non-prescription foot orthoses are foot which are fabricated in average sizes and shapes in an attempt to match the most prevalent sizes and shapes of feet within the population without utilizing a three dimensional representation of the plantar foot of the individual receiving the orthosis.
Prevention
Custom-made orthotics supports not only the arch as a whole, but also each individual bone and joint that forms the arch. It is not enough to use an over-the-counter arch support, as these generic devices will not provide the proper support to each specific structure of the arch and foot. Each pronated foot?s arch collapses differently and to different degrees. The only way to provide the support that you may need is with a custom-made device. This action of the custom-made orthotic will help to prevent heel spurs, plantar fasciitis, calluses, arch pain, and weakness of the entire foot.
What Exactly Is Calcaneal Apophysitis?
Overview
Pain in the heel of a child's foot, typically brought on by some form of injury or trauma, is sometimes Sever's Disease. The disease often mimics Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon may contribute to Sever's Disease by pulling excessively on the growth plate of the heel bone. This condition is most common in younger children and is frequently seen in the active soccer, football or baseball player. Sport shoes with cleats are also known to aggravate the condition. Treatment includes calf muscle stretching exercises, heel cushions in the shoes, and/or anti-inflammatory medications. Consult your physician before taking any medications.
Causes
Young athletes typically sustain the injury due to repeated stress caused by running and jumping. Partaking in any high speed sports can thus partly provoke the condition, such as football, rugby, basketball, hockey or track athletics. Crucially the injury is linked to overuse, so exercising with fatigued leg muscles, without a suitable warm up, or beginning a new strenuous physical activity are all risk factors. Placing excessive weight or pressure on the heel can also cause the injury. Another factor related to Sever's disease is overpronation, a biomechanical error that makes the foot roll too far inwards.
Symptoms
This is a condition that affects the cartilage growth plate and the separate island of growing bone on the back of the heel bone. This growth plate is called the physeal plate. The island of growing bone is called the apophysis. It has the insertion attachment of the Achilles tendon, and the attachment of the plantar fascia. This island of bone is under traction from both of these soft tissue tendon and tendon-like attachments.
Diagnosis
Sever?s disease can be diagnosed based on the symptoms your child has. Your child?s doctor will conduct a physical examination by squeezing different parts of your child?s foot to see if they cause any pain. An X-ray may be used to rule out other problems, such as a broken bone or fracture.
Non Surgical Treatment
When the condition flares, it is treated with activity limitation, medication to reduce inflammation (such as ibuprofen [Advil] or naproxen [Aleve]), shoe inserts, heel lifts, cold packs, and sometimes casting when it becomes especially severe. Sever condition is generally a self-limited problem that usually improves within a year.
Recovery
Sever?s disease is self-recovering, meaning that it will go away on its own when the foot is used less or when the bone is through growing. The condition is not expected to create any long-term disability, and expected to subside in 2-8 weeks. The disease may also take several years to stop, because it is often triggered by growing too fast. It is more common in boys, although occurs in girls as well. The average age of symptom onset is 9-11.
Pain in the heel of a child's foot, typically brought on by some form of injury or trauma, is sometimes Sever's Disease. The disease often mimics Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon may contribute to Sever's Disease by pulling excessively on the growth plate of the heel bone. This condition is most common in younger children and is frequently seen in the active soccer, football or baseball player. Sport shoes with cleats are also known to aggravate the condition. Treatment includes calf muscle stretching exercises, heel cushions in the shoes, and/or anti-inflammatory medications. Consult your physician before taking any medications.
Causes
Young athletes typically sustain the injury due to repeated stress caused by running and jumping. Partaking in any high speed sports can thus partly provoke the condition, such as football, rugby, basketball, hockey or track athletics. Crucially the injury is linked to overuse, so exercising with fatigued leg muscles, without a suitable warm up, or beginning a new strenuous physical activity are all risk factors. Placing excessive weight or pressure on the heel can also cause the injury. Another factor related to Sever's disease is overpronation, a biomechanical error that makes the foot roll too far inwards.
Symptoms
This is a condition that affects the cartilage growth plate and the separate island of growing bone on the back of the heel bone. This growth plate is called the physeal plate. The island of growing bone is called the apophysis. It has the insertion attachment of the Achilles tendon, and the attachment of the plantar fascia. This island of bone is under traction from both of these soft tissue tendon and tendon-like attachments.
Diagnosis
Sever?s disease can be diagnosed based on the symptoms your child has. Your child?s doctor will conduct a physical examination by squeezing different parts of your child?s foot to see if they cause any pain. An X-ray may be used to rule out other problems, such as a broken bone or fracture.
Non Surgical Treatment
When the condition flares, it is treated with activity limitation, medication to reduce inflammation (such as ibuprofen [Advil] or naproxen [Aleve]), shoe inserts, heel lifts, cold packs, and sometimes casting when it becomes especially severe. Sever condition is generally a self-limited problem that usually improves within a year.
Recovery
Sever?s disease is self-recovering, meaning that it will go away on its own when the foot is used less or when the bone is through growing. The condition is not expected to create any long-term disability, and expected to subside in 2-8 weeks. The disease may also take several years to stop, because it is often triggered by growing too fast. It is more common in boys, although occurs in girls as well. The average age of symptom onset is 9-11.
Working With An Achilles Tendon Rupture
Overview
 The Achilles tendon is the largest and strongest tendon in the human body. The Achilles tendon connects the heel bone (calcaneus) to the muscles at the back of the calf (using gastrocnemius and soleus muscles). The synchronous function of the tendon and calf muscles is critical for activities like jumping, running, standing on the toe, and climbing stairs. When climbing stairs or running, the forces within the tendon have been measured and indicate that the structure is able to withstand at least 10 times the body weight of the individual. The function of the Achilles tendon is to help raise your heel as you walk. The tendon also assists in pushing up the toes and lifting the rear of the heel. Without an intact Achilles tendon, almost any motion with the ankle (for example, walking or running) is difficult.
The Achilles tendon is the largest and strongest tendon in the human body. The Achilles tendon connects the heel bone (calcaneus) to the muscles at the back of the calf (using gastrocnemius and soleus muscles). The synchronous function of the tendon and calf muscles is critical for activities like jumping, running, standing on the toe, and climbing stairs. When climbing stairs or running, the forces within the tendon have been measured and indicate that the structure is able to withstand at least 10 times the body weight of the individual. The function of the Achilles tendon is to help raise your heel as you walk. The tendon also assists in pushing up the toes and lifting the rear of the heel. Without an intact Achilles tendon, almost any motion with the ankle (for example, walking or running) is difficult.
Causes
The causes of an Achilles tendon rupture are very similar to Achilles tendinitis. Causes include. Running uphill. Running on a hard surface. Quickly changing speeds from walking to running. Playing sports that cause you to quickly start and stop.
Symptoms
When the Achilles tendon ruptures a loud bang or popping sound may be heard. The person may feel that they have been hit or kicked in the back of the lower leg and often they will look over their shoulder to see who or what has hit them. This is quickly followed by the sudden onset of sharp pain in the tendon and a loss of strength and function. If a complete rupture has occurred it may not be possible to lift the heel off the ground or point the toes. Often the degree of pain experienced, or lack of it, can be inversely proportional to the extent of the injury, ie a partial rupture may in fact be more painful than a complete rupture.
Diagnosis
In diagnosing an Achilles tendon rupture, the foot and ankle surgeon will ask questions about how and when the injury occurred and whether the patient has previously injured the tendon or experienced similar symptoms. The surgeon will examine the foot and ankle, feeling for a defect in the tendon that suggests a tear. Range of motion and muscle strength will be evaluated and compared to the uninjured foot and ankle. If the Achilles tendon is ruptured, the patient will have less strength in pushing down (as on a gas pedal) and will have difficulty rising on the toes. The diagnosis of an Achilles tendon rupture is typically straightforward and can be made through this type of examination. In some cases, however, the surgeon may order an MRI or other advanced imaging tests.
Non Surgical Treatment
Non-surgical treatment of Achilles tendon rupture is usually reserved for patients who are relatively sedentary or may be at higher risk for complications with surgical intervention (due to other associated medical problems). This involves a period of immobilization, followed by range of motion and strengthening exercises; unfortunately, it is associated with a higher risk of re-rupture of the tendon, and possibly a less optimal functional outcome. 
Surgical Treatment
The surgical repair of an acute or chronic rupture of the Achilles tendon typically occurs in an outpatient setting. This means the patient has surgery and goes home the same day. Numbing medicine is often placed into the leg around the nerves to help decrease pain after surgery. This is called a nerve block. Patients are then put to sleep and placed in a position that allows the surgeon access to the ruptured tendon. Repair of an acute rupture often takes somewhere between 30 minutes and one hour. Repair of a chronic rupture can take longer depending on the steps needed to fix the tendon.
Prevention
Here are some suggestions to help to prevent this injury. Corticosteroid medication such as prednisolone, should be used carefully and the dose should be reduced if possible. But note that there are many conditions where corticosteroid medication is important or lifesaving. Quinolone antibiotics should be used carefully in people aged over 60 or who are taking steroids.